In our recent article, Providing Telephonic and Virtual Care Requirements as part of COVID-19 Precautions, available on HCCI’s COVID-19 Information Hub, we highlighted the requirements of virtual visits. We also provided an overview of the 1135 Telehealth Waiver as part of the president’s emergency declaration during the country’s current public health emergency.
We realize this is a challenging time for Home-Based Providers, and the Home Centered Care Institute (HCCI) is committed to supporting the field by providing timely information so you can make the best decisions for your practice. In response to recent questions, we’ve outlined more information below to clarify additional questions you may have.
Q: What are the current Evaluation and Management (E/M) codes that can be billed for when the services are provided via telehealth under the 1135 Waiver?
A: Here are the appropriate E/M codes:
- Office/Outpatient CPT code range 99201-99215
- Transitional Care Management CPT codes 99495 and 99496
- Advance Care Planning CPT codes 99497 and 99498
- Annual Wellness Visits HCPCS codes G0438 and G0439
- Administration of caregiver-focused health risk assessment instrument CPT code 96161
- Telehealth consultations ED or initial inpatient visits HCPCS code range G0425-G0427
- Follow-up inpatient telehealth consultations in hospitals or SNF’s HCPCS range G0406-G0408
For a complete list of CPT codes, please refer to Medicare’s list of telehealth services
HCCI is awaiting official guidance from CMS on whether Home-Based Practices that historically bill only for home or domiciliary visits should be concerned about a potential heightened audit risk if they use the office visit code set during this pandemic. We realize, however, that many Home-Based Practices are choosing to use the set office visit code, in the interim, to maintain their practice. Our recommendation is to review all the facts before making the best decision for your practice and consider contacting your local Medicare Administrator Contractor (MAC) for specific guidance.
Q: What Place of Service (POS) and modifiers are required to bill for telehealth services?
A: For services furnished via telehealth, report Place of Service (02) for telehealth.
Per the CMS FAQs & The Medicare Learning Network’s March 20th update, CMS does not generally require additional or different modifiers on Medicare claims for telehealth services furnished under these waivers, except in the following three instances:
- GQ – Telehealth services are furnished via asynchronous (store and forward) technology as part of a federal telemedicine demonstration project in Alaska and Hawaii
- GT – Telehealth services are furnished under CAH Method II (Via interactive audio and video telecommunication systems)
- G0 – Telehealth services are furnished for the purposes of diagnosis and treatment of an acute stroke
As an example of when receiving guidance from your local MAC is beneficial, a practice in Indiana reached out to their MAC (i.e., WPS Government Health Administrators) and was advised to use modifiers for telehealth claims.
Q: How do I contact and confirm who my local MAC is?
A: CMS has a contractor directory and map on their website that allows you to search by state to confirm your MAC along with links to each contractor’s site where you can find their Provider Contact Center phone number. You will need to call your MAC directly to request clarification on proper billing for home visits under the 1135 waiver. They may refer you to a specific governance email, however, HCCI is aware that practices are generally receiving timely responses within a few days.
It’s also important to note the requirement for practices to use an interactive audio and video telecommunications system that permits real-time communication between the provider and the patient at home even under the telehealth waiver. This means you cannot bill for an E/M visit via telehealth for phone call audio-only. However, under the U.S. Department of Health and Human Services (HHS), the Office of Civil Rights (OCR) Notification of Enforcement Discretion relaxed HIPAA requirements so that providers may use platforms such as Apple FaceTime, Skype, Zoom, the WhatsApp, etc., as a form of two-way audio and video telecommunications. Doxy.me, a free HIPAA-compliant telemedicine platform that allows for two-way audio and video interaction with patients and caregivers, is another option. Consider checking with your Electronic Health Record (EHR) vendor as they may have technologies available for video visits, too.
If you are providing virtual services to patients via phone call audio-only, you must refer to the Virtual Check-in Codes (requirements detailed in previous HCCI article), or use other forms of reimbursement, such as care management services (e.g., Chronic Care Management) to bill for your time.
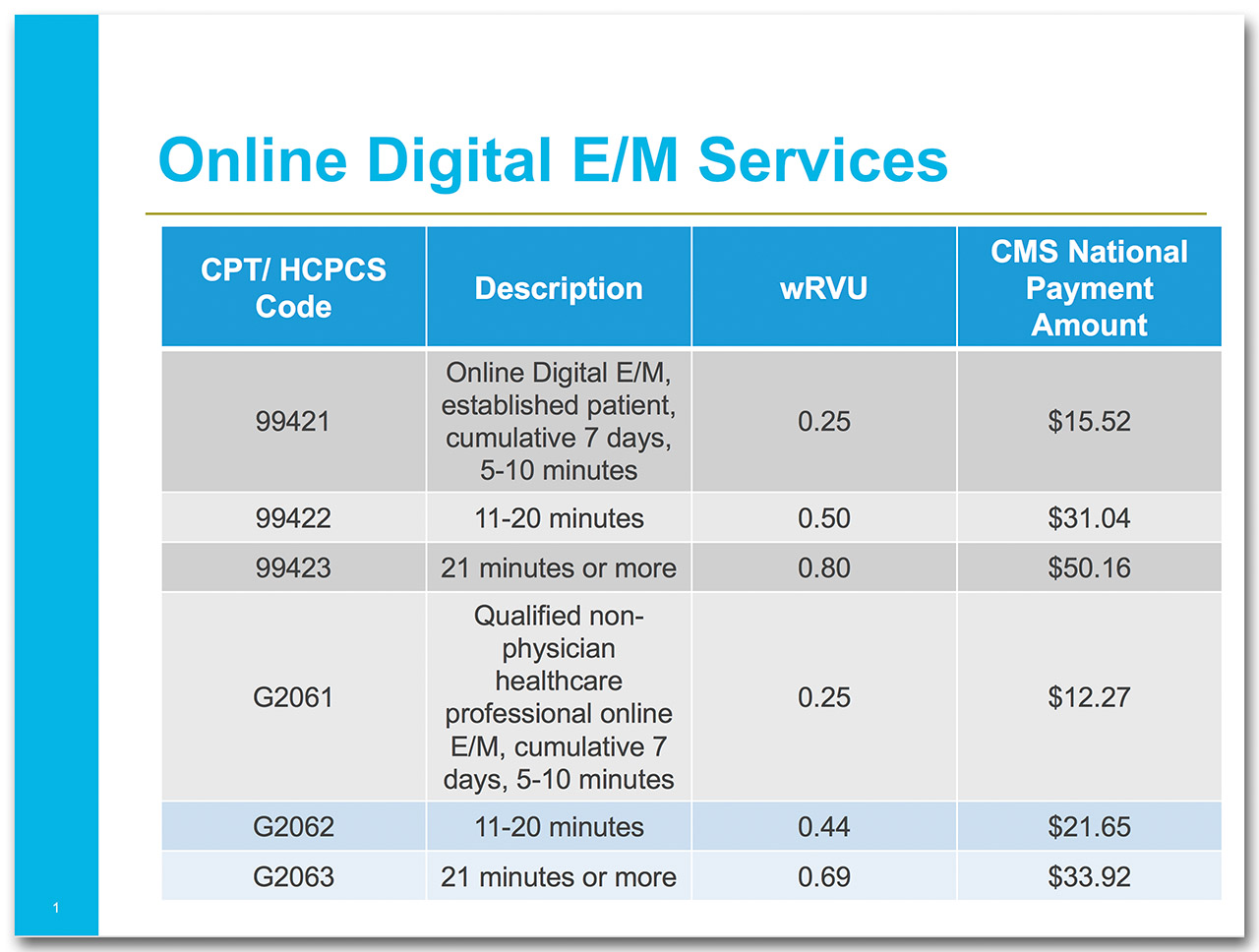
The E-visits codes, which capture time over a 7-day period for communicating and reviewing patient information on a digital communication platform, such as a patient portal or secure email, are listed below in an HCCI chart for easy reference:
For additional information, refer to the CMS General Provider Telehealth and Telemedicine Tool-kit, or contact a member of the HCCIntelligence™ Hotline staff at 630-283-9222 or email [email protected].
Disclaimer: This information is current as of 3/23/2020. Coding regulations are subject to change annually, and COVID-19 guidelines are changing daily. Please note for the purposes of the Home-Based Primary Care (HBPC) population: The Home Centered Care Institute (HCCI) focuses our content on CMS guidelines relevant for traditional Medicare billing.